The healthcare system at large has experienced a notable increase in the share of providers and health systems assuming financial risk for the total cost of care. The rise of these value-based models has historically been driven by the Centers for Medicare & 医疗补助云顶集团(CMS), with programs focused on populations of high cost and cost variability—specifically, 65岁以上有慢性疾病者. 然而, 随着时间的推移, state Medicaid programs and commercial payers have begun introducing value-based contracts of their own, 包括那些关注高危儿童的研究.
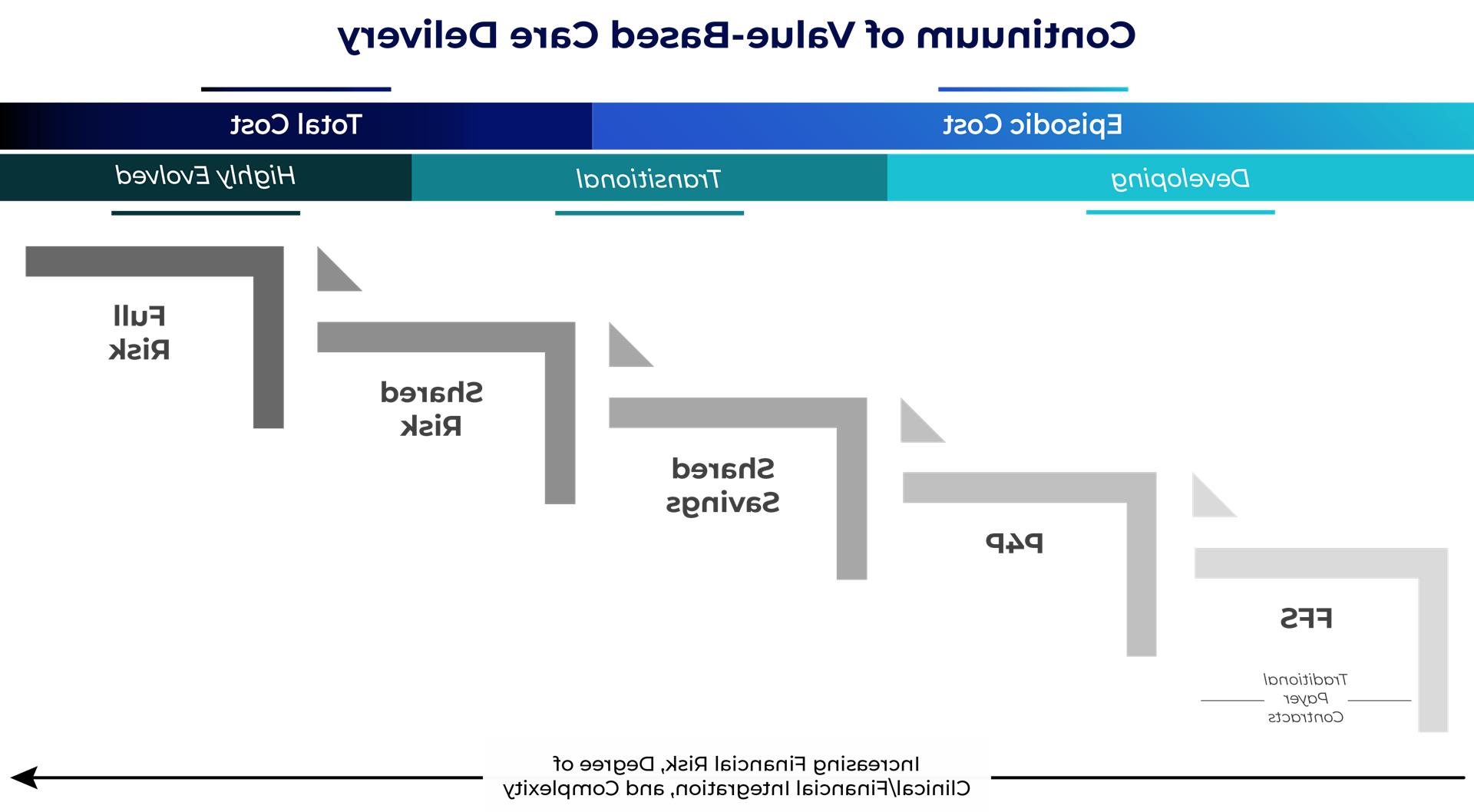
The term “value-based care” encompasses a broad continuum of care delivery models, and each requires a different degree of financial risk assumption, 如图1所示.
- 低风险模型包括那些关注偶发成本的模型, 比如绩效工资(P4P)和共享储蓄. These structures offer an opportunity for providers to earn financial bonuses based on quality performance without any downside risk.
- More evolved value arrangements may follow a shared-risk or full-risk structure, 在这种情况下,供应商在财务上有更大的潜力, 但是作为回报, must also assume downside risk in the event healthcare spending exceeds a predetermined amount or quality thresholds are not met.
图1
在儿科机构内, a majority of existing risk programs are based on episodic costs and include limited, 或没有, 下行金融风险. 然而, given that most nationally recognized children’s health systems have either clinically or financially integrated physician organizations, they are able to coordinate care effectively and succeed under pay-for-performance or shared savings arrangement types. Only a select few pediatric systems have progressed across the value continuum to assume full financial risk for a defined population (these include Texas Children’s Hospital and Cook Children’s Health Care System, 他们都制定了自己的健康计划).
独特的挑战导致价值逐渐被接受
Pediatric organizations have been slower to adopt shared- and full-risk models for a variety of reasons, 包括:
- Metrics that appropriately and accurately measure pediatric outcomes and quality of care are limited. 这些指标在哪里可用, they are often difficult for payers to implement and operationalize when compared to traditional, adult-focused指标.
- Patients treated in these pediatric systems are often high-acuity, complex cases. 这对传统的价值模式提出了挑战, 哪些通常以初级保健提供者为中心.
- A lack of adequate pediatric post-acute care providers makes it difficult for systems to coordinate and manage care beyond the acute care setting.
- 一旦程序被开发出来, pediatric systems may have difficulty developing a reliable methodology to assess and stratify their pediatric population by risk profile—a key component for success under a total risk arrangement.
- 操作上, pediatric systems may lack fully integrated electronic health records that can share data across a broader network of independent specialists and providers.
These compounding challenges have led many pediatric health systems and payers to conclude that global risk assumption, 正如它目前呈现的那样, 不能转移到儿科人群吗.
也就是说, most pediatric organizations are already investing in capabilities such as advanced care management, 的家庭看护模型, 数字健康. 然而, many of these organizations have developed this infrastructure out of necessity to improve operations, 支持病人吞吐量, 并释放住院病人的能力. 换句话说, they’re delivering value for payers but aren’t being reimbursed or recognized for their services.
因此, pediatric systems should first focus on aligning current reimbursement terms to account for any support services they are providing that may not be directly reimbursable under traditional fee-for-service contracts. This may include care management or coordination services through strong inpatient and affiliated outpatient networks, or virtual follow-up and e-consult programs used to reduce readmissions. 来支持他们的观点, pediatric systems will need to quantify how these efforts reduce costs, 创建额外容量, 解析访问约束, 减少使用, 减少再入院人数. 基于这些产生的节省, the organization must be prepared to approach payer partners and propose a payment structure that will ensure compensation for value-added services.
儿科系统应该主动评估价值准备情况
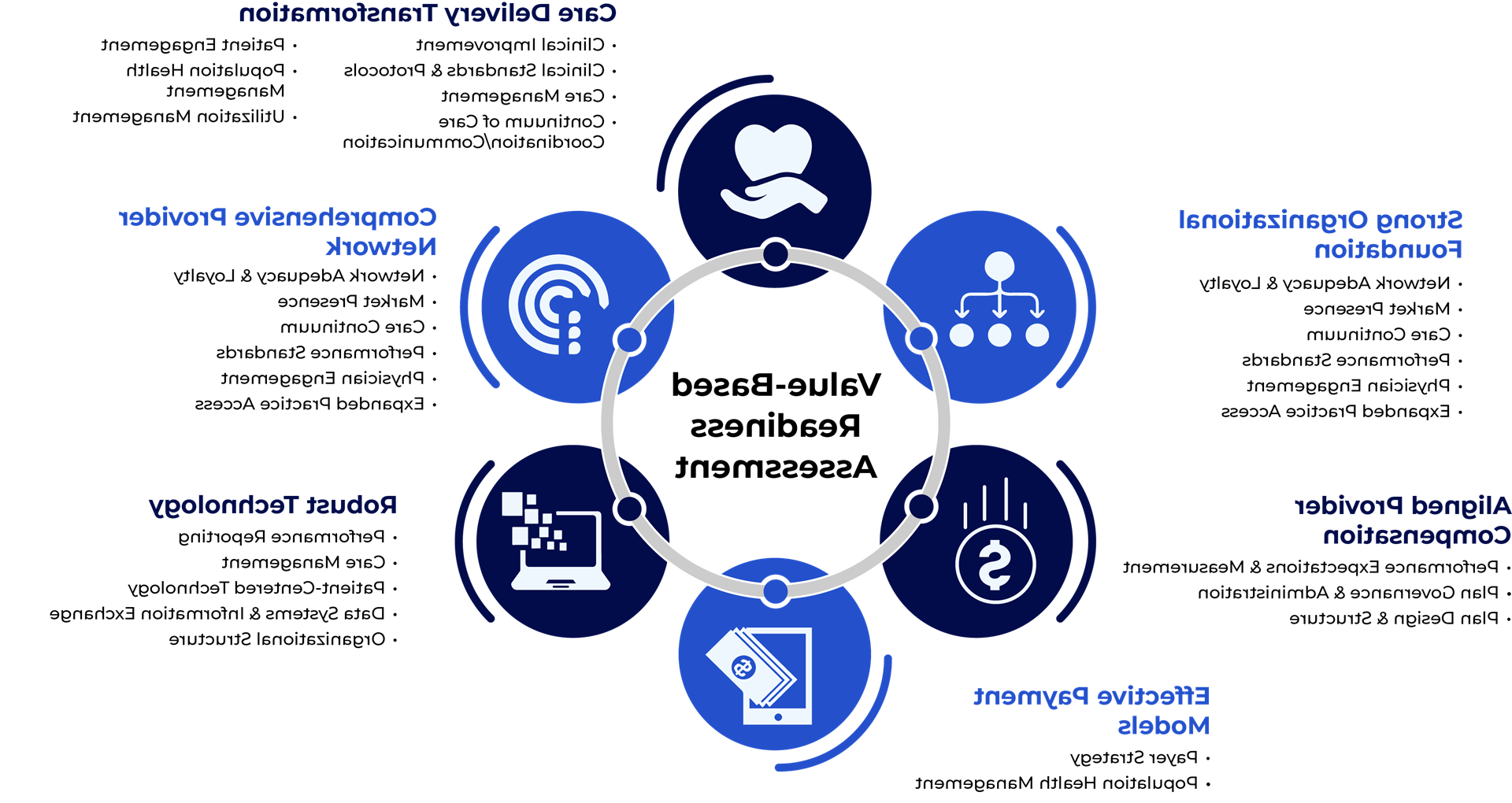
For pediatric organizations that are prepared to move to the next phase of risk assumption, leadership will first need to conduct an assessment to determine the degree of organizational readiness. For instance, 心电图 evaluates value-based readiness on a set of key criteria, as shown in figure 2.
图2
While full-risk models may not be immediately viable for most organizations, pediatric systems need to proactively evaluate their readiness to assume financial risk and then develop a strategy that aligns reimbursement with organizational goals, 临床和/或运营投资, 预计的市场压力. 心电图期望在儿科护理中风险的吸收是渐进的, 但我们也预见到,患者的敏锐度不断提高等趋势, 对综合行为健康云顶集团的需求, and the growing focus on early intervention will continue to push the conversation forward.
如果方法正确,准备充分, value-based care can offer pediatric systems a unique opportunity to enhance quality and outcomes for their highest-risk patients while generating incremental revenue and positioning their organization for long-term success.
了解更多云顶集团的儿科战略和管理护理团队
编辑:马特·马斯林
出版于2024年1月17日